
Utilizing Group Cellphones to Promote Healthy Practices

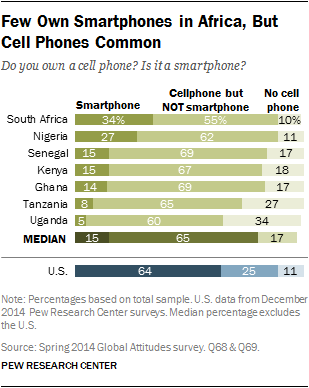
The increasing proliferation of cellphones in Africa brings an opportunity to leap-frog off technological development to innovative mobile interventions. Our case study takes place in Nigeria, with a cellphone proliferation rate of 89%. MHealth is an innovative approach towards the integration of technology and health interventions. However, mHealth is limited for those without cell phone access; generally the most vulnerable like women in rural communities or the illiterate (40.4% of the population over the age of 15 cannot read and write in Nigeria[1]). Therefore, Partners for Development and Dr. Valerie L. Flax, with her team of researchers from the University of North Carolina, provided groups of women with cellphones to research their effectiveness in disseminating and encouraging vulnerable populations to adhere to recommended health practices.
The researchers targeted women-microcredit clients. These women had received small loans and were already integrated into a group dynamic with other microcredit clients where peer support and accountability was highly valued for microfinance program success. PfD’s intervention utilized the pre-existing small groups of women-microcredit clients for the purpose of our health promotion program; by linking social networks together with health information via text and voice messaging we are able to encourage communication and behavior change. The research found that integrating group counseling and cell phone messaging increased the likelihood of women to adhere to breastfeeding recommendations.
Dr. Flax performed a second round of research to analyze the feasibility and acceptability of group cellphones used to promote optimal breastfeeding practices for women’s microcredit groups within Nigeria. During this research, in each microcredit group, one woman was provided a low-cost cell-phone that received text/voice messages weekly on breastfeeding information. The woman responsible for the cell phone was asked to disseminate the information to her group within a week
Key findings from the target group (195 microcredit clients whose babies were born during intervention) include:
- 68% of the time, breastfeeding messages were usually shared in the small groups rather than individually
- 44% of groups met at least once a week to discuss the breastfeeding messages
- 59% of the small groups performed songs and dramas about the breastfeeding messages every week
- 58% of women trusted the messages and were motivated to try recommended practices
- 64% said the group phone worked well or very well
- 35% felt they had the support to carry out the breastfeeding recommendations
With regards to the feasibility and acceptability of providing a single cell phone to a group, focus group discussions showed unanimous neutral or positive feelings towards the single cell phone holder. Reports also show the information was shared promptly. Moreover, women continued to share what they learned about breastfeeding to their family and friends. In congruence with prior research, women in the target group who met at least once a week were more likely to exclusive breastfeed in comparison to women who never met with their group. As we can see, utilizing mobile health promotion in a group setting is a feasible, acceptable and worthwhile approach.
In conclusion, despite Nigeria’s high cellphone penetration rate, women tend to have less access to cellphones and thereby mobile health promotion technology. Therefore, this tactic of targeting women who already have group dynamics formed within their microcredit program was effective in promoting optimal breastfeeding practices through the use of a group cell phone. This research is groundbreaking in exemplifying the feasibility of integrating mobile health technology into groups of the most vulnerable peoples.
At PfD, we are dedicated to delivering local solutions with sustainable outcomes. As seen in this exemplified program, women and children are at the forefront of our programming. Learn more about PfD’s work promoting lifesaving and cost-effective recommended maternal health practices in our blog, https://pfd.org/building-on-the-microcredit-platform-for-better-child-health/. And read more about our work in Nigeria with maternal health here https://pfd.org/the-question-of-quality-comprehensive-respectful-and-rights-based-maternal-health/
Flax V.L., Negerie M., Ibrahim A.U., Leatherman S., Daza E.J. & Bentley M.E. (2014) Integrating group counseling, cell phone messaging, and participant-generated songs and dramas into a microcredit program increases Nigerian women’s adherence to international breastfeeding recommendations. The Journal of Nutrition 144, 1120-1124
[1] https://www.cia.gov/library/publications/the-world-factbook/fields/2103.html

The Question of Quality: Comprehensive, Respectful, and Rights-Based Maternal Health
Imagine that you’re a young, pregnant woman. Imagine that you have to walk five miles to even get to the doctor. You arrive at the clinic, only to sit in a small, hot, overcrowded waiting room for four or more hours. When you finally do get to see a nurse, she mocks your accent, or your clothes. She scolds you for not coming in sooner, and makes you feel ashamed. Your understanding was that it was a free exam, but then you are asked to go to the pharmacy to buy gloves for the nurse. The nurse pricks your finger and says she’s testing you for a disease. You think you’ve heard of this disease, and you heard it kills people. You’re scared of it, but she doesn’t say more – doesn’t say if she thinks you might have it or if it will hurt your baby. You’re given a confusing mix of pills that are bitter tasting, and told that the clinic is out of some. The nurse says you should come back next week to get these, and that you should come back for another exam in 2 months.
Would you return to the health facility?
For many women in the developing world, this example closely resembles their experience. Each year, over 300,000 women die in pregnancy and childbirth, 99 percent of them in the developing world. For every woman who dies of pregnancy-related complications, 20 to 30 more suffer from related on-going conditions which may permanently affect their normal functioning –additional 6 to 9 million women per year. Maternal health advocates, researchers, and providers are committed to ending human rights abuses and promoting skilled and dignified care. Together, we can make comprehensive, respectful, and rights-based maternal health care available to all.
Maternal mortality and morbidity are the tragic result of a myriad of compounding factors. 75% of maternal deaths are caused by severe bleeding, infections, high blood pressure during pregnancy, complications from delivery, and unsafe abortion. Other deaths are often caused by or associated with other diseases such as malaria or AIDS. Delivering at a medical facility with a skilled health care worker present is critical should these complications arise, but often they can be avoided altogether if a woman attends antenatal care visits. However, only 40% of women in low-income countries complete the recommended number of antenatal care visits.
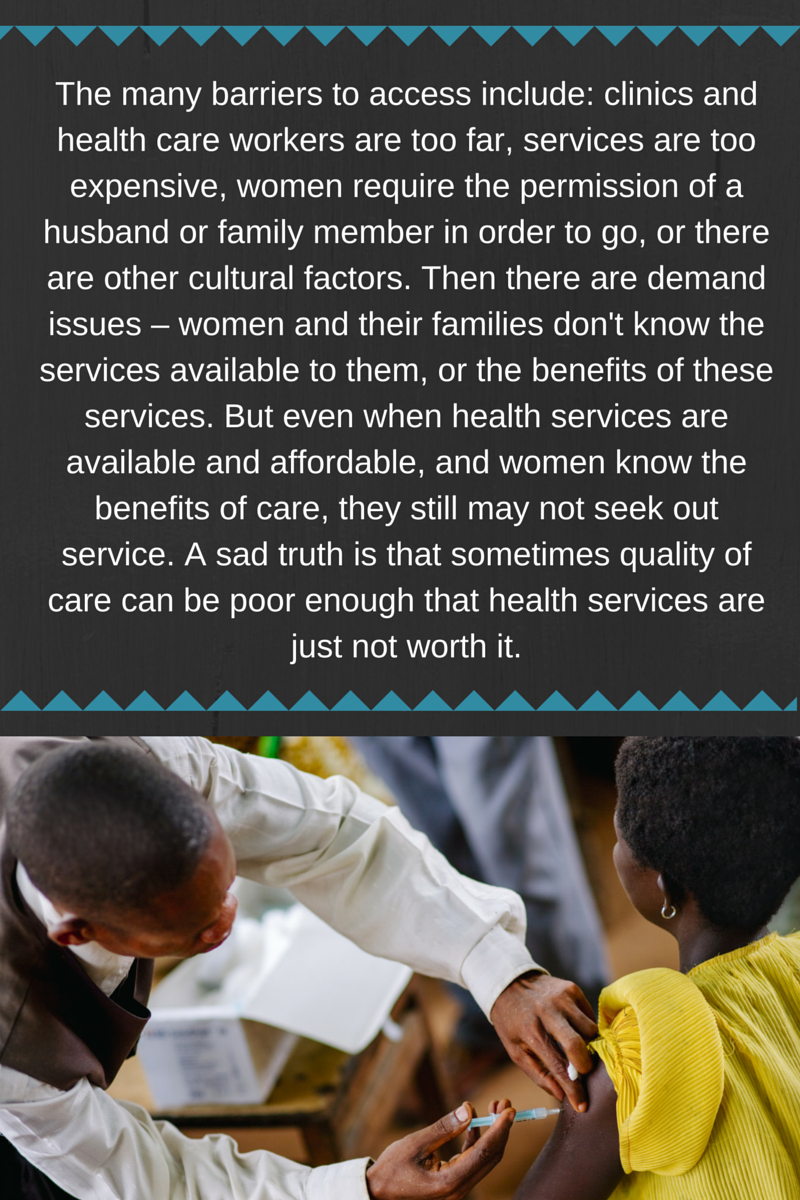
As the example above illustrates, accessing care for some women can not only be difficult, it can be intimidating, humiliating, and scary. Unsurprisingly, receiving poor care makes women less likely seek health care out in the future. This is why it’s crucial to not only provide access (by making healthcare close and affordable), to educate women, their families, and their communities about the importance of maternal health care, but also to work with health clinics and health workers to ensure quality of care – the respectful, comprehensive, and competent care that every human deserves.
At PfD, we deliver integrated programs that address the nuanced reality on the ground. In Nigeria, we not only provide education to women, their families, and communities and engage with key community leaders to change behavior. We also work with health care providers to ensure that they have the knowledge and resources to provide quality care. PfD worked to deliver improved maternal, newborn, and child health services through the training and mentoring of health care personnel, including nurses and midwives, community health extension workers, and community based healthcare volunteers. PfD trained nurses and midwives on quality of care and trained health care workers on Balanced Counseling Strategy which improves client-provider interactions and client satisfaction. The results of this project speak for themselves – In the first year of the project, 15,562 women attended at least one session of antenatal care during pregnancy – by the end of the project over 44,000 did. This represents an increase of over 280%.
Through the Scale-up of Prevention of Mother-to-Child Transmission and Pediatric HIV/AIDS services in Delta State, Nigeria, PfD built the capacity of health facilities, training health workers to provide quality HIV testing and counseling, integrating Prevention of Mother-to-Child Transmission and HIV care into antenatal care services, and upgrading and equipping a laboratory to service as a comprehensive treatment hub. PfD trained health care workers and pregnant women received HIV testing and counseling. PfD also facilitated testing of pregnant women for HIV.
PfD is committed to the idea that no woman should be in danger because she gives birth, which is why we’re joining the global community in calling on the UN Secretary General to recognize April 11th as the International Day for Maternal Health and Rights. Together with the UN community we can make comprehensive, respectful, and rights-based maternal health care available to all. To sign the petition,click here. Follow the discussion at #IntlMHDay and through PfD’s social media updates. To learn more about our work to promote maternal health and healthy communities, click here.
April 6th, 2016, by Katie Baczewski, PfD Program Officer

Nigeria is the seventh most populated country in the world, and nearly 50% of the population lives below the poverty line. As a result of Nigeria’s weak health system and high prevalence of poverty, the country suffers from extremely high mortality and morbidity rates among vulnerable people, especially children under-five years of age and women of child-bearing age. People living in the northern states of the country generally suffer from poorer health and health services.
In response, Partners for Development (PfD) began working in Bauchi and Sokoto states to strengthen the relationship between community institutions and healthcare delivery systems and improve overall primary health care services and management provided by local and state governments.
To achieve this, PfD trained and mentored health care personnel who were responsible for delivering family planning and reproductive, maternal, newborn and child health services, including nurses, midwives and community health workers and volunteers. PfD also established committees within each ward and each LGA, building the capacity of each to promote health seeking behaviors within their communities.
PfD developed and integrated health counseling services, education about best health practices, and the identification of community health workers in order to mobilize communities and perpetuate the success of established activities. In particular, PfD’s work with community health volunteers in disseminating health messages and providing referrals to health facilities significantly contributed to the overall success of the project.
Ultimately, PfD’s community-based approach to development once again resulted in the successful improvement of health services in the target areas of Bauchi State. PfD’s focus on capacity building and sustainable programming allowed for significant achievements in the quality and accessibility of healthcare in the LGAs.
This work was completed by Partners for Development (PfD) under the JSI-led and USAID funded Targeted States High Impact Project (TSHIP) in Nigeria’s Bauchi and Sokoto states. Under TSHIP, PfD won a sub-grant to support initiatives in five Local Government Areas (LGAs) in Bauchi that focused on institutional capacity building, delivery of health services, and community participation in and promotion of health-seeking behaviors. Read more: The Role and Impact of Partners for Development (PFD) in the Targeted States High Impact Project (TSHIP).


Today, on the 67th anniversary of the creation of the World Health Organization (WHO), individuals and organizations have the opportunity to highlight initiatives around the globe that promote better health. Thus today, PFD shines the spotlight on our work in Sexual Reproductive Health and Rights (SRHR) around the globe.
 Improving Sexual Reproductive Health Rights (SRHR) is essential for the physical, mental and social wellbeing of individuals, especially women. While progress has been made, women frequently suffer from unequal gender relations, limiting their physical agency and ability to negotiate safe sex. In the developing world, as many as 222 million women do not have access to any methods of contraception (WHO 2015). The consequences of this are far reaching including maternal mortality, physiological trauma, higher rates of STDs and higher numbers of infant mortality. Thus, SRHR is a crucial human rights issue that has long-term implications on global health and international development as a whole.
Improving Sexual Reproductive Health Rights (SRHR) is essential for the physical, mental and social wellbeing of individuals, especially women. While progress has been made, women frequently suffer from unequal gender relations, limiting their physical agency and ability to negotiate safe sex. In the developing world, as many as 222 million women do not have access to any methods of contraception (WHO 2015). The consequences of this are far reaching including maternal mortality, physiological trauma, higher rates of STDs and higher numbers of infant mortality. Thus, SRHR is a crucial human rights issue that has long-term implications on global health and international development as a whole.
PFD has an extensive history with reproductive health programming in both Africa and Asia. In Cambodia, for example, beginning in 2004, PFD partnered with the United Nations Fund for Population Activities (UNFPA) to provide access to quality reproductive health education and services. The program was primarily targeted towards young people ages 10-24 in Kratie Province. PFD also integrated HIV/AIDS prevention into our SRHR programing. This collaboration increased effectiveness and efficiency by reaching the youth with education on both the key issues of reproductive health and disease prevention simultaneously.
Since its initial work in Cambodia, PFD has expanded its reproductive health targeted programming toNigeria. Working in some of the most challenging areas in Nigeria, PFD has successfully implemented integrative reproductive health programming with microfinance initiatives. In Bauchi State, a northern province in Nigeria, PFD has expanded its health systems project Targeted States High Impact Project (TSHIP) in collaboration with John Snow International (JSI) and funded by United States Agency for International Development (USAID). TSHIP fosters improvement of reproductive and family planning services through grassroots techniques and local partnerships. PFD has combined these programs with income generating activities that facilitate business skills and small enterprise development, improving the personal autonomy and livelihoods of poor women.
TSHIP Outcomes as of December 2014:
- Provided Reproductive Health (RH) counseling to 37,528 to males and females or reproductive age.
- Increased the completion rate of individual RH referrals to 74%.
- Provided intermittent preventive treatment (IPT) for malaria to 57,067 pregnant women.
- Aided 10,286 births with skilled attendants.
What can you do?
You too can make an impact on World Health Day. Show your support by sharing on social media and tagging @Partners4dev on Twitter or following us on Facebook. Support Partners for Development’s work in health around the globe and donate here.

Women across the world face many challenges to equality, from access to economic, health, and education resources, to violence within communities and households. To commemorate International Women’s Day on March 8th and this year’s theme Make it Happen, PFD will be honoring the achievements of women around the globe.
Investing in women important not only because it ensures equality, but also because investing in women can produce positive externalities, expanding the impact of each dollar invested.
PFD works across the globe in three main sectors:
 Economic Growth
Economic GrowthPFD works with and supports microfinance organizations and institutions around the world, to increase access to credit for underserved populations. In these programs, over 91% of borrowers were women. PFD has found that when these entrepreneurial women generate additional income, a large portion is reinvested into the family, often paying for school fees for their children. In Nigeria, PFD and Lift Above Poverty Organization (LAPO), a local microfinance organization, further assist women to invest in their families by offering to fund scholarships to daughters of women microfinance clients. According to the World Bank, one additional year of education for girls results in lower infant mortality and higher future incomes. By funding scholarships for girls, PFD and LAPO are also investing in future generations.
On International Women’s Day and always we honor these women.
Health  PFD trains community health volunteers to spread health information within their communities. Women who receive this training not only are able to implement changes for themselves, but they also can implement healthier practices for their families. The women are trained to spread the information in the communities and by reaching out to other women, can indirectly reach their families. In Cambodia, for instance, from 2012-2014, PFD trained over 1,500 village health volunteers in malaria health education, a majority of whom were women. In 2013, there were almost 300,000 maternal deaths worldwide related to pregnancy and childbirth. PFD works to prevent deaths by increasing access to skilled health services. In 2013 in Nigeria, with the support of PFD and local partners, 45,501 women attended at least one antenatal care visit and 19,483 women were assisted by skilled delivery attendants during childbirth.
PFD trains community health volunteers to spread health information within their communities. Women who receive this training not only are able to implement changes for themselves, but they also can implement healthier practices for their families. The women are trained to spread the information in the communities and by reaching out to other women, can indirectly reach their families. In Cambodia, for instance, from 2012-2014, PFD trained over 1,500 village health volunteers in malaria health education, a majority of whom were women. In 2013, there were almost 300,000 maternal deaths worldwide related to pregnancy and childbirth. PFD works to prevent deaths by increasing access to skilled health services. In 2013 in Nigeria, with the support of PFD and local partners, 45,501 women attended at least one antenatal care visit and 19,483 women were assisted by skilled delivery attendants during childbirth.
USAID reported in its 2012 “Gender Equality and Female Empowerment Policy” that ensuring women farmers have the same access to land, technology, and credit, crop yields can be increased “as much as 30 percent and feed an additional 150 million people”. In Benin, PFD is implementing USDA’s Growing Resources for Enhanced Agricultural Enterprises and Nutrition (GREEN). GREEN Project is working with farmers associations to increase farm revenues and productivity by building knowledge through trainings, providing information on markets and price information, and increasing access to credit. In 2013 and 2014, through GREEN, PFD and its partners were able to reach over 48,413 farmers, around half of whom were women, with trainings on farming techniques, markets and value chains, and on business development skills. Additionally, PFD integrated its micro-credit methodology into GREEN, increasing access to credit to farmers so they can implement the newly learned skills. Of the 4,680 loans made to farmers, and over 2,250 of the loans were given to women.
On International Women’s Day and always we praise the hard work and perseverance of these women.
How can you Make it Happen?
Support Girls’ Education: Help educate and empower the next generation of young women by contributing to PFD here and designating the Nigerian Scholarship fund for Girls.
Give your Support: Support PFD to develop new, innovative programs that support women and girls around the globe here.
Use your voice: Post about women’s social, economic & political achievements using the hashtag #makeithappen or #womensday! Don’t forget to also use the PFD handle @Partners4Dev so we can share your message too!
Spread the word: Repost this blog on social media to help support the movement.

Throughout all of December we will be sharing stories from our staff, board, partners, and others from around the globe. We can’t wait to share all of the hopeful, engaging, and positive stories from our work. We will be using the hashtag #IamPfD on Facebook, Twitter and LinkedIn.

Donate Now
Be sure to share the posts that you find engaging and inspiring with friends and family and don’t forget to donate and take an #unselfie of you making a donation and share it with us and use the #IamPfD for a chance to win prizes from PfD.
The CDC reports that improved water, sanitation and hygiene could potentially prevent 9.1% of the global disease and 6.3% of all deaths. Therefore, PFD and UNICEF –are teaming up in Nigeria to Strengthening Capacity of Local Institutions to Drive Community-Centered WASH Service Delivery. The project will help improve access to safe drinking water and improve sanitation facilities in three southern states of Nigeria.
 Less than 20 % of households in the three PFD target areas are using improved water sources and less than half of households in these areas have improved sanitation facilities (Nigerian Ministry of Health). Drawing from past experience working in Nigeria and implementing WASH programming in Cambodia, PFD will work with local organizations to empower communities through trainings and other tools to create sustainable improvements providing
Less than 20 % of households in the three PFD target areas are using improved water sources and less than half of households in these areas have improved sanitation facilities (Nigerian Ministry of Health). Drawing from past experience working in Nigeria and implementing WASH programming in Cambodia, PFD will work with local organizations to empower communities through trainings and other tools to create sustainable improvements providing
water, sanitation and hygiene (WASH) services.
Key to PFD efforts are two things: sustainability and integration.
Building a strong foundation is vital to sustainability. The foundation for this program: Community Water, Sanitation and Hygiene Committees (WASHCOM). PFD will work within local communities of six Local Government Areas (LGA) each in Delta, Edo, and Ekiti states to organize and empower 600 WASHCOMs through training, mentoring, and other methods. The training of trainers is a key part of building capacity to ensure sustainability. State level workshops will train project staffs and volunteers to facilitate the project interventions in their communities and continuous mentoring of trainees will allow for the internalization of their new skills. Additionally, by creating a forum in each community, community members will have a space to share and learn best practices for the implementation of WASH activities. The forums will also provide a foundation so each community can continue to address WASH problems and adapt to changing needs in the future.
Going forward, WASHCOMs will serve as a platform for integrated programing. With a community structure in place, PFD and UNICEF will be able to address different community needs, providing reproductive health and family planning messaging, a platform for community peacebuilding and social bonding, and trainings for facilitation.
We know that integrated programming works: PFD’s programs done in unison have proven to be far more successful together than they are alone. When PFD integrated breastfeeding and maternal health messaging into its microfinance program in Nigeria, researchers found the number of women who exclusively breastfeed their infants increased.
The key to these successful sanitation interventions is not just the visible infrastructure, but also the corresponding education and community awareness. Working in the isolated and underserved northeast region of Cambodia, PFD improved rural access to safe water and sanitation in a country where less than 30 percent of the rural population has access to safe water and less than 10 percent to adequate sanitation.
Essential to this process is working with and through local organizations – PFD’s modus operandi. By strengthening the capacity of local organizations and equipping local CBOs to manage the work it both increases the level of community participation and provides a foundation for local ownership. Within the water and sanitation programs in Cambodia, PFD integrated health, nutrition, and food security activities, recognizing the interconnected nature of development and the need a multifaceted approach.
Follow the links to learn more about PFD‘s programs in WASH and health, and our work inCambodia and Nigeria!

Originally published on DevEx through the Healthy Means Campaign
By: Dr. Valerie Flax
In resource-constrained settings, early and exclusive breastfeeding prevents infant and child deaths from diarrhea and other infectious diseases, supports normal growth, and improves cognitive performance throughout childhood. Yet, optimal breastfeeding practices are declining globally, with less than half of the world’s newborns benefitting from early breastfeeding and about one-third exclusively breastfed for the first six months of life. Low-cost and effective strategies to improve breastfeeding behaviors in underserved areas are urgently needed.
Photo 1: A credit officer leads a discussion on breastfeeding during a monthly microcredit meeting in Bauchi State, Nigeria
how to download norton antivirus on windows 8 on 8 using complete setup guide
Two ways to efficiently reach out to a large number of women with messages on breastfeeding are through microfinance programs and cell phone messages. Incorporating health programs into microfinance takes advantage of the social networks and social support inherent in group activities and that type of support is needed to change breastfeeding behaviors. Cell phone messages are a great way to increase the number of repeated contacts with women who most need encouragement to breastfeed. Partners for Development and researchers from the University of North Carolina tested these ideas in northeast Nigeria by integrating group breastfeeding promotion and cellphone messaging into a microcredit program. The integrated program increased the number of women who started breastfeeding early and who exclusively breastfed their infants for six months.
We reached out to women participating in a microcredit program, a system in which small business owners, often women, receive loans to begin or advance their enterprise. Small groups of five to seven friends, neighbors and/or relatives join the program together and meet regularly with several other small groups to repay their microloans.
Every month, credit officers led discussions about breastfeeding during microcredit meetings. Sessions covered recommendations for early and exclusive breastfeeding, benefits of following breastfeeding recommendations, breastfeeding techniques and timing for introducing complementary foods. Key messages from the meetings were sent as text and voice messages to phones that were given to small-group leaders, who were instructed to share the messages. Group members selected some messages to be dramatized or turned into songs and performed at monthly microcredit meetings.
Giving phones to small groups of women was a key component of the program. It pushed them to gather together to review and discuss the messages. Many groups also shared the messages with other community members, thereby facilitating a shift in social norms related to breastfeeding practices. One phone holder explained her experiences, “This is a trust given to me that when a message comes to the phone, I must try my best to share it with women in the group. I don’t only share with members of the group, but include neighbors. Even during casual discussions, as we pass time, I find a way to chip in something about our program to attract them. This way they have accepted the messages I share that come through the phone.”
By building innovative face-to-face and mobile health components onto a microcredit program, we can spread messages to women in the groups and their friends and neighbors, greatly broadening the impact. The intervention could be scaled up in Nigeria and adopted more widely given that nearly 200 million women, many of childbearing age, are involved in microfinance globally. Assuming that each woman participating can have an impact on 5 of her family members and friends, this type of program, if scaled up, has the potential to benefit 1 billion worldwide.
Author Valerie L. Flax, PhD, Assistant Professor of Nutrition in the UNC Gillings School of Global Public Health, led the study through the Partners for Development with funding from the Alive and Thrive small grants program. The study involved women from communities in the Bauchi State in northern Nigeria. This trial was registered at clinicaltrials.gov as NCT01352351. The Journal of Nutrition published the research in July 2014. Partners for Development is a non-profit organization with community-driven programs in Africa and Southeast Asia. PFD works with vulnerable populations in the areas of health, agriculture, food security, livelihoods, and microfinance.